
Just saying “shingles” is like saying Beetlejuice 3 times. No one wants to think about having a shingles outbreak. We all know someone who’s had shingles (herpes zoster), and it’s not pretty. About 1.2 million people in the US are diagnosed each year (Albrecht, 2019). People normally complain mostly of the pain. The intense, fire-like, unique but miserable discomfort that the rash brings is what people remember. But before we discuss shingles, we have to talk about chicken pox. Yes. They’re sibling diseases. The first phase of shingles is chicken pox. Then, shingles later brings its wrath.
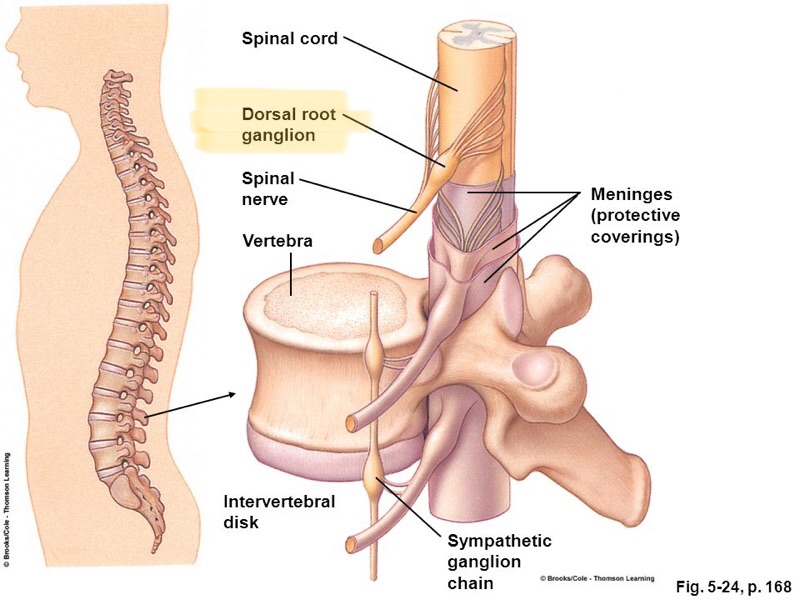
Did you have chicken pox as a kid? According to the CDC, 99% of adults over 40 have had chicken pox, even if they don’t remember having it. Well, guess what? Your virus never really “went away.” Your rash did, but the virus lives in your FOREVER. Yes, f.o.r.e.v.e.r. The chicken pox virus, also called varicella zoster, lies dormant in either the right or the left side of your spinal cord at ONE nerve root (called the dorsal root ganglion; picture below). This place of rest determines where you will get shingles, if you ever get an outbreak. So, for example, if the chicken pox virus decides to rest at the second nerve root (in the neck) on the right side, you’ll have shingles blisters in your scalp, on your face, or even into your eye, but only on the right side. If it lies dormant in your lower back, say at the first lumbar vertebrae on the left, you’ll get the blisters on your hip/ lower back/ just above your genitalia on the left side of your body only. Why does the virus pick a specific nerve root? That’s yet to be discovered. Answer that question for us medical folks, and you’ll be a popular human being. PLEASE refer to the diagram below of what we call “dermatomes.” This is a skin map of how spinal nerves manifest sensations and diseases on the skin.
FYI: If you have a rash on both sides of the body and you think it may be shingles, you’re wrong. Shingles cannot cross your midline. It’s only on one side of the body.
OKAY, this is the who, what, when, where, and why of shingles.
Who: Anyone. The most likely patient to have shingles is someone elderly who recently has undergone a lot of stress, a new and major life change, or someone whose immune system has recently taken a dive. I will say, most of my shingles patients are elderly. In fact, 50% of folks who live until 85 years old can report that they’ve had shingles (Albrecht, 2019).
What: Shingles is what we call a “vesicular” rash. See picture below. The rash has a bright red base with fluid-filled blisters or “vesicles.” The rash is actually not the first symptom of shingles, though. A tingling, burning, itching sensation is usually the first sign you’re about to have a rash. The symptoms occur on the area you’ll expect to see blisters form over the next day or two. If you feel like someone is holding a lighter to your skin and you’re also wanting to itch it, shingles may be in your very near future. Sorry, Charlie.


right side.
When: Every. Single. One. of my patients who present to my office with shingles admits to recently undergoing a significant life stressor. Some have an immune depletion (like someone undergoing treatment for active cancer or someone with lupus, for instance), but seriously the most common patient is or has recently been horribly stressed. The virus senses when the body is in a stressed state, and it takes advantage of the weakness. My last two patients with shingles (one was in her 30s and the other in her 50s), had recently moved from one house to another. Moving is a big ordeal. You lose sleep over it, undergo financial changes, have a lot of organization challenges, and are embarking upon the unknown. Shingles senses this all-around fatigue and the outbreak occurs.
Where: I touched on this earlier, but let’s delve into the details. Your spinal cord has nerves exit from the right and left of your spine between each vertebrae. On the right and the left sides of the spine are nerve roots. The shingles virus (after chicken pox occurs) sits and waits in one of these nerve roots, usually for decades (sadly, though, some children can and do get shingles). The virus lies dormant and hibernates like a bear in the wintertime. The lucky ones never get a shingles outbreak. But many, many folks do, hence why a vaccine was created. Anyway, look below at some pictures to see what I mean by “where.”

Why: Sort of the same as “when.” Some very unlucky folks have shingles more than once in their lifetime. These people are usually immunocompromised and/or regularly and highly stressed. If you get shingles but don’t feel significantly stressed, and can’t really pinpoint a new or changing life event in the last month, I would speak with your PCP. You may have an issue with your immune system, and it’s worth some investigating. Blood work will be a good start, along with a lengthy review of your current/ past/ family medical history.
Is shingles contagious? Not really. Well, yes, but rarely. You cannot give shingles to someone else. Here is the when your shingles rash will affect someone else: let’s say someone who has never had the chicken pox and has never been vaccinated against chicken pox touches your actively seeping/draining blisters OR breathes in your respiratory droplets while you have the shingles rash. They will get chicken pox, not shingles, from you. I have actually seen this in my clinical rotations as a student. A 5-month old infant (not yet old enough to get her chicken pox vaccine) got chicken pox because her grandmother who took care of her daily had shingles. Grandma held her granddaughter on her right hip, where her blisters were broken out, and chicken pox shortly ensued in the little one. Pearl of wisdom: have shingles? Keep the blisters covered with bandages or dressings, and keep away from infants and immunocompromised people.
Shingles complications
As if the burning, itching, painful rash wasn’t enough, there exists a condition called “post-herpetic neuralgia” or PHN. It’s essentially pain, itching, sensitivity, and tingling where your rash WAS, for sometimes up to 12 months post-outbreak. It’s not a fun time. It’s truly defined as significant, persistent discomfort for at least 4 months after rash onset (Cleveland Clinic, 2019). About 10-15% of shingles sufferers complain of PHN, and half are 60+ years old. People who receive the shingles vaccine are MUCH less likely to have PHN. There is medication for this— the approved treatments are gabapentin and Lyrica, both in the same drug class. They treat the nerve pain associated with shingles. Opiates are not indicated for this type of pain. PHN is a unique kind of nerve pain, as I mentioned before, and opiates just aren’t designed for this disorder. Gabapentin is your hero, here, usually because it’s less expensive than Lyrica and it’s normally approved on insurances more readily than Lyrica.
There exists vision and neural complications with shingles, so if you have fever, headache, delirium, blurred vision, or sudden loss of vision, visit the ER immediately.
Treatment
Treatment works best when it’s initiated within 72 hours of symptom presentation. An antiviral pill is the only medication that treats shingles (acyclovir, famcyclovir, and valacyclovir). No matter the agent selected, you’ll take it for 7 days. Treatment is aimed to prevent the rash from worsening and to prevent post-herpetic neuralgia.
Shingles Vaccination
There are two vaccines for shingles. Since 2006, Zostavax has been available. Until recently, it was the only option on the market. It’s one injection, and it lasts you about 5 years. Its efficacy at time of injection lessens with age. Are you 80 and get the Zostavax? You won’t have an impressive protection against the rash. It’s indicated for healthy folks over 60. We say healthy folks should get it, meaning that you aren’t knowingly immunocompromised. According to the CDC, on average, Zostavax reduces your chance of getting shingles by 51%.
In 2017, Shingrix became available. It’s so popular, it’s currently on backorder. Pharmacies have waiting lists for patients to be called in for their shots. Adults 50 and older should get this vaccine. In fact, this is the shingles vaccine favored among the 2 available. It comes in 2 doses, with 2 to 6 months separating the injections. Those 2 doses give over 90% protection against the outbreak. Protection remains at 85% within the first 4 years of getting vaccinated. You can get the Shingrix if you’ve had shingles before, if you’ve already had the Zostavax, or aren’t even sure if you had chickenpox.
Check with your insurance carrier on vaccine coverage. If you have any questions about the vaccine, check the CDC website. The link is listed in my references below.
If you’re a young sprout reading this and had the chickenpox vaccine instead of the actual virus, you’re quite unlikely to get shingles. You would get the shingles if at some point your immune system depleted several years after your chicken pox immunization, you then contracted chicken pox, then developed shingles after that (VERY if-and-then…). Therefore, with strong vaccination rates, shingles should begin to diminish in prevalence, with the exception of those with poor immune systems and those otherwise healthy individuals who foolishly chose to not be vaccinated.
Moral of the story: you don’t want shingles. It hurts, it’s miserable, and it can have complications. Get vaccinated. If you don’t want to wait for the newest Shingrix, get the Zostavax. Some protection is better than none! Seek immediate medical attention if you think you have shingles, because the sooner you initiate treatment, the better. Oh, and avoid significant stressors as you age. Easier said than done, I know. But truly, this is the biggest indicator in my experience for shingles outbreak potential in a healthy adult. May you never get shingles, and God bless you if you do.
References:
Albrecht M and Levin M. Epidemiology, clinical manifestations, and diagnosis of herpes zoster. 2019 November. Retrieved December 8, 2019 from https://www.uptodate.com/contents/epidemiology-clinical-manifestations-and-diagnosis-of-herpes-zoster?search=shingles&source=search_result&selectedTitle=2~150&usage_type=default&display_rank=2.
Albrecht M. Treatment of herpes zoster in the immunocompetent host. 2018 December 10. Retrieved December 8, 2018 from https://www.uptodate.com/contents/treatment-of-herpes-zoster-in-the-immunocompetent-host?search=shingles&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1
CDC. What everyone should know about shingles vaccines. 2019. Retrieved December 7 2019 from https://www.cdc.gov/vaccines/vpd/shingles/public/index.html.
Photo sources:
Shingles of back: https://familydoctor.org/condition/shingles/
Shingles of chest: https://www.webmd.com/skin-problems-and-treatments/shingles/ss/slideshow-shingles-myths-facts
Dermatomes: http://www.sciencedirect.com
Main photo: Shutterstock
